

This is a difficult question to answer. The etiology of each of these chronic illnesses remains, alas, a mystery that we have yet to conclusively solve.
That being said, it is very important that we solve them. Why? Because baby-boomers (a very large portion of the American population) are headed into geriatric conditions. Among the most common of these is fibromyaligia. It is to pain management, what alzheimer’s and frontotemporal dementia are to neurology.
What we do know is that pain, fibromyalgia, depression and chronic fatigue syndrome often share common symptoms:
- sleep disturbance (usually long-term)
- excessive stress levels
- psychological repercussions/detriments from sleep loss, excessive stress, and other factors
- reduced capacity for activities of daily living (ADLs), resulting in reduced cardiovascular exercise and resultant hypofitness
All these factors result in:


We also know that although the above symptoms seem to correlate with inflammation, research has shown a demonstrated lack of local inflammation in these shared co-morbidities (common co-occurences). In addition, as inflammation does not occur, anti-inflammatories do not help.
Further answers to this question have filled many textbooks (and been part of ongoing debate in pain management) due to unexplained etiology: if we could figure out the biological pathways that develop the disease, we would at least be closer to a definitive understanding of the commonalities between these diseases. We could then address and treat them definitively.
To my knowledge, the closest we have come to a definitive etiology of fibromyalgia is as follows (if someone knows differently, PLEASE correct me):
- Fibromyalgia can be considered a discrete condition, as well as a construct. This helps explain how/why individuals have multifocal pain and other somatic symptoms in spite of the lack of nociceptive input (i.e., peripheral damage/inflammation) that adequately accounts for the pain.
- The primary abnormality, identified to date in fibromyalgia and related pain syndromes, is an increased gain (as in a volume control turned up) in central nervous system pain processing (i.e., secondary hyperalgesia/allodynia).
- It is likely that this “turning up the volume” on pain and sensory processing is in part due to increased levels of excitatory neurotransmitters (e.g., glutamate, substance P), and/or low levels of inhibitory neurotransmitters (serotonin, norepinephrine, GABA, cannabinoids).
- Analgesics that work well for “peripheral/nociceptive” pain syndromes (e.g., NSAIDS, opioids), are largely ineffective in fibromyalgia.
- The most effective classes of drugs in fibromyalgia are centrally acting analgesics (e.g., triciyclics, serotonin re-uptake inhibitors, “SNRI”s, and anticonvulsants (calcium channel blockers).
- Nonpharmacologic therapies such as education, exercise, manual therapy, and cognitive behavioral therapy are very effective in fibromyalgia and are typically underutilized in routine clinical practices. [2]


Diffuse pain (11/18 points on the body – see diagram above) is the hallmark of fibromyalgia, and this is notably absent in depression and chronic fatigue syndrome. It is also absent, in this pattern, in myofascial pain syndrome (MPS), which tends to be more localised, and also tends to be more functionally oriented. In the fibromyalgia patient, the common complaint is that, “I hurt all over.” The tissue feels very soft and broken-down, versus taut bands and knots of MPS. However, they do sometimes coincide. (See Devin Starlanyle and Mary Ellen Copeland’s “Fibromyalgia & Chronic Myofascial Pain.”)


As to how this has been established in case studies, please see the below table:

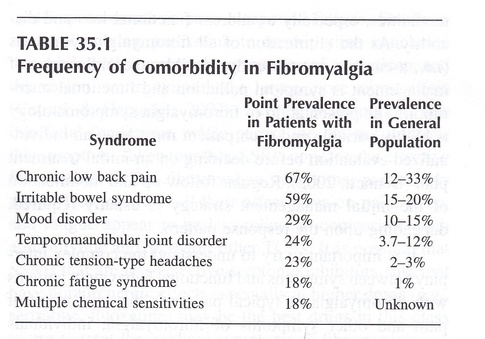
So, what does this all mean?
- Sleep quality/quantity is interrupted.
- There is usually a level of sustained stress and psychological distress.
- There is a discrepancy of diagnostic criteria: pain with fatigue and psychological distress, versus fatigue and psychological distress, versus psychological distress alone. Granted, cases may change over time (see above diagragm) but the primary characteristics of each individual’s case remain unique in these criteria.
To show this in another way, here’s a current diagram for commonalities that would produce these common symptoms:

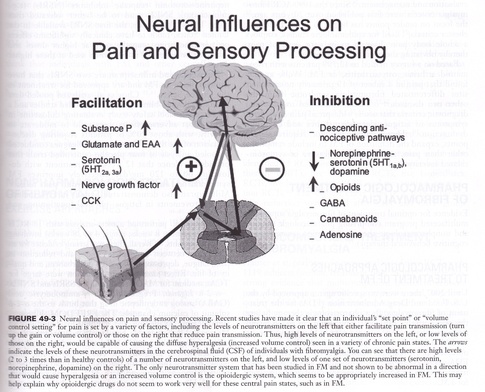
This would help to explain the commonalities of:
- sleep disturbance ~/= fatigue
- depression
- low pain threshold (easily triggered pain)
- functional compromise
In addition, it may explain why:
- Amitryptaline/Nortryptaline (SSRI) are helpful in treating many of these common symptoms, via increased levels of available serotonin and norepinephrine/noradrenaline levels in overall tissue.
- Lyrica/Neurontin (Ca Channel blockers) are helpful to treat many of these common symptoms, via reduced central excitability in signal (especially pain signal) processing.
It is agreed, though, in interdisciplinary pain management, that effective therapy for ALL of these conditions MUST include:
- Appropriate pharmacologic prescriptions, and
- Cognitive Behavioral Therapy, to learn triggering deactivation and new coping mechanisms: to mediate pain perception and subsequent neuromodulation.
The following is further noted as helpful:
- Physical therapy: Begin an appropriate “start low, go slow” low-impact cardiovascular exercise program, such as aquatic therapy or other low-impact mechanisms. This maximises tissue metabolism and ultimate tone.
- Massage therapy: This modality maximises efficiency of circulatory return and tissue metabolism, in order to enable the tissue to respond to functional demands and short/long-term capabilities (much like physical therapy).
- Acupuncture: This modality reduces overall CNS (central nervous system) hyperactivation and restores CNS stability. Some studies vary as to the effectiveness of this modality, but observed results are more consistent. In practice, it has shown to help with patient’s ability to comply with functional demands, perhaps due to lowering levels of CNS hyperalgesia. [6]
I wish I had more definitive information to convey. In pain management circles, this is what we’ve got so far. Know, however, that we’re working on it, ardently.
I’ll update as I’m able to.
- Essentials of Pain Medicine, 3d Edition; 2011; Benson, Raja, et al.; pg. 346
- Ibid., pg.350
- fibromyalgia points of pain diagram
- Weiner’s Pain Management: A Practical Guide for Clinicians (American Academy of Pain Management), 7th edition; 2007; Mark V. Boswell, B. Eliot Cole; pg. 497
- Essentials of Pain Medicine, pg.347
- What can neuroscience conclude about acupuncture? by Adriano Stephan on CogSci