First, it’s good that one see a doctor, even if that doctor is unable diagnose the problem. If there is no diagnosis of hernia, however, below is some information concerning the muscle-strain aspect of this issue.
This presentation of symptoms is consistent with a strain of the external oblique muscle of the abdominals (shown in red, below):
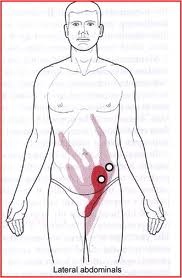
The strain can result in a trigger point, which is a hyperirritable locus, or “knot,” within a taut muscle band that refers (sends) pain to a location distant to it (pictured as circles in the above picture). The trigger point we’re concerned with is located in the bands of external oblique about 1-2″ above the inguinal ligament (groin line). This is the lower circle in the picture. If you lean forward a bit, to relax this muscle, you can feel the fibers of this muscle going in a diagonal line:
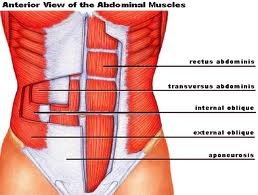
You can palpate (feel) this muscle quite easily, as it is very near the surface of the body:
After you’ve found the taut, guitar-string-like band of external oblique, do the following:
-
Apply heat to the area first. This will help relax the muscle fibers and flush pain chemicals from the tissue. This also dilates the blood/lymph vessels and brings fresh blood to the area, making it easier to “dissolve” the trigger point (#3, below).
-
Run your fingers up and down the band (guitar-string) of the external oblique muscle to find a “knot” (trigger point) or point of “exquisite tenderness.”
-
Push on the trigger point for up to 1-2 minutes. It should feel as if it is “dissolving,” softening, or simply becoming less sensitive. Keep the pressure on until it feels done “dissolving.”
You can also use ice packs along the lower ribs to decrease motor nerve over-activation to this muscle.
(For more information on the Abdominal external oblique muscle, please click on the highlighted text.)
Next, It is important to take the external oblique muscle through its full range of motion following trigger point release. The following stretches are helpful:
- A full (careful, non-painful) lunge:
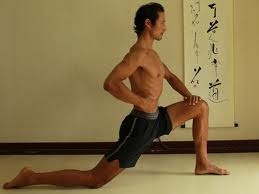
Please be careful not to take the front knee more forward than that side’s foot (which can strain that side’s knee). Observe the upright calf angle here on the forward leg.

Observe that the person reaches up and back over the side being stretched, which directly stretches external oblique
If there is pain during these stretches, fall back to a position where there is no pain, just a sensation of “pull/stretch.” Then relax/breathe until you don’t feel the pain anymore.
If there is sharp pain at any point during these exercises, STOP immediately and ice the area of sharp pain. Wait until all pain or tension in the area has passed. Then try again, going much slower and easier.
If these techniques do not work within one week of daily practice, more interventional techniques (trigger point injection or nerve block) may be in order, which a pain management specialist can determine.
In my practice, I have found that roughly half of the cases respond quickly and well to these simple techniques. More severe strains (most often sports injuries, and minus hernia diagnoses) require the deeper interventional techniques mentioned above.




