
Chronic pain, depression, fibromyalgia and chronic fatigue all seem to feed off each other but which came first? What is the root of this debilitation?
This is a difficult question to answer. The etiology of each of these chronic illnesses remains, alas, a mystery that we have yet to conclusively solve.
That being said, it is very important that we solve them. Why? Because baby-boomers (a very large portion of the American population) are headed into geriatric conditions. Among the most common of these is fibromyaligia. It is to pain management, what alzheimer’s and frontotemporal dementia are to neurology.
What we do know is that pain, fibromyalgia, depression and chronic fatigue syndrome often share common symptoms:
- sleep disturbance (usually long-term)
- excessive stress levels
- psychological repercussions/detriments from sleep loss, excessive stress, and other factors
- reduced capacity for activities of daily living (ADLs), resulting in reduced cardiovascular exercise and resultant hypofitness
All these factors result in:

We also know that although the above symptoms seem to correlate with inflammation, research has shown a demonstrated lack of local inflammation in these shared co-morbidities (common co-occurences). In addition, as inflammation does not occur, anti-inflammatories do not help.
Further answers to this question have filled many textbooks (and been part of ongoing debate in pain management) due to unexplained etiology: if we could figure out the biological pathways that develop the disease, we would at least be closer to a definitive understanding of the commonalities between these diseases. We could then address and treat them definitively.
To my knowledge, the closest we have come to a definitive etiology of fibromyalgia is as follows (if someone knows differently, PLEASE correct me):
- Fibromyalgia can be considered a discrete condition, as well as a construct. This helps explain how/why individuals have multifocal pain and other somatic symptoms in spite of the lack of nociceptive input (i.e., peripheral damage/inflammation) that adequately accounts for the pain.
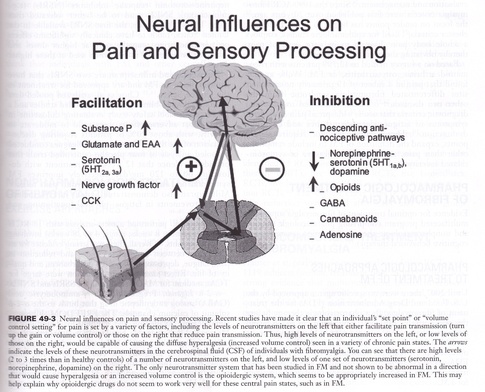
- The primary abnormality, identified to date in fibromyalgia and related pain syndromes, is an increased gain (as in a volume control turned up) in central nervous system pain processing (i.e., secondary hyperalgesia/allodynia).
- It is likely that this “turning up the volume” on pain and sensory processing is in part due to increased levels of excitatory neurotransmitters (e.g., glutamate, substance P), and/or low levels of inhibitory neurotransmitters (serotonin, norepinephrine, GABA, cannabinoids).
- Analgesics that work well for “peripheral/nociceptive” pain syndromes (e.g., NSAIDS, opioids), are largely ineffective in fibromyalgia.
- The most effective classes of drugs in fibromyalgia are centrally acting analgesics (e.g., triciyclics, serotonin re-uptake inhibitors, “SNRI”s, and anticonvulsants (calcium channel blockers).
- Nonpharmacologic therapies such as education, exercise, manual therapy, and cognitive behavioral therapy are very effective in fibromyalgia and are typically underutilized in routine clinical practices. [2]

Diffuse pain (11/18 points on the body – see diagram above) is the hallmark of fibromyalgia, and this is notably absent in depression and chronic fatigue syndrome. It is also absent, in this pattern, in myofascial pain syndrome (MPS), which tends to be more localised, and also tends to be more functionally oriented. In the fibromyalgia patient, the common complaint is that, “I hurt all over.” The tissue feels very soft and broken-down, versus taut bands and knots of MPS. However, they do sometimes coincide. (See Devin Starlanyle and Mary Ellen Copeland’s “Fibromyalgia & Chronic Myofascial Pain.”)

As to how this has been established in case studies, please see the below table:
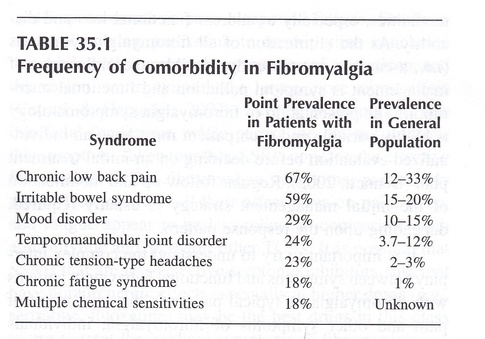
So, what does this all mean?
- Sleep quality/quantity is interrupted.
- There is usually a level of sustained stress and psychological distress.
- There is a discrepancy of diagnostic criteria: pain with fatigue and psychological distress, versus fatigue and psychological distress, versus psychological distress alone. Granted, cases may change over time (see above diagragm) but the primary characteristics of each individual’s case remain unique in these criteria.
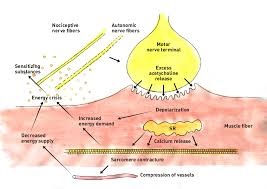
To show this in another way, here’s a current diagram for commonalities that would produce these common symptoms:
This would help to explain the commonalities of:
- sleep disturbance ~/= fatigue
- depression
- low pain threshold (easily triggered pain)
- functional compromise
In addition, it may explain why:
- Amitryptaline/Nortryptaline (SSRI) are helpful in treating many of these common symptoms, via increased levels of available serotonin and norepinephrine/noradrenaline levels in overall tissue.
- Lyrica/Neurontin (Ca Channel blockers) are helpful to treat many of these common symptoms, via reduced central excitability in signal (especially pain signal) processing.
It is agreed, though, in interdisciplinary pain management, that effective therapy for ALL of these conditions MUST include:
- Appropriate pharmacologic prescriptions, and
- Cognitive Behavioral Therapy, to learn triggering deactivation and new coping mechanisms: to mediate pain perception and subsequent neuromodulation.
The following is further noted as helpful:
- Physical therapy: Begin an appropriate “start low, go slow” low-impact cardiovascular exercise program, such as aquatic therapy or other low-impact mechanisms. This maximises tissue metabolism and ultimate tone.
- Massage therapy: This modality maximises efficiency of circulatory return and tissue metabolism, in order to enable the tissue to respond to functional demands and short/long-term capabilities (much like physical therapy).
- Acupuncture: This modality reduces overall CNS (central nervous system) hyperactivation and restores CNS stability. Some studies vary as to the effectiveness of this modality, but observed results are more consistent. In practice, it has shown to help with patient’s ability to comply with functional demands, perhaps due to lowering levels of CNS hyperalgesia. [6]
I wish I had more definitive information to convey. In pain management circles, this is what we’ve got so far. Know, however, that we’re working on it, ardently.
I’ll update as I’m able to.
- Essentials of Pain Medicine, 3d Edition; 2011; Benson, Raja, et al.; pg. 346
- Ibid., pg.350
- fibromyalgia points of pain diagram
- Weiner’s Pain Management: A Practical Guide for Clinicians (American Academy of Pain Management), 7th edition; 2007; Mark V. Boswell, B. Eliot Cole; pg. 497
- Essentials of Pain Medicine, pg.347
- What can neuroscience conclude about acupuncture? by Adriano Stephan on CogSci
What is the science behind Trigger Point deep muscle massage? Does it work? How many sessions does it take before you feel relief?
The answer to this question will include current, state-of-the-art research, as well as my and my colleagues’ clinical experience over several decades. I will address each of the three questions in sequence.
1) What is the science behind trigger point deep muscle massage?
There are several theories for the etiology/pathophysiology of trigger points and myofascial pain syndrome. Research continues on each, as none have yet been decisively proven.[1][2] Massage therapy (MT) has been studied extensively, and has been shown to produce objective effects most notably in those bodily systems which interact locally with the myofascial (muscle and connective tissue) systems.[3] These include the local circulatory systems, local and central nervous systems, and the lymphatic system within the immediate vicinity of the area worked on. It should be noted that the fascial structures, which encapsulate the contractile structures and tissues, exert mechanical forces upon the other associated structures, thus affecting their physiological function. MT (specifically ischemic compression and friction massage) has been shown to be effective in releasing myofascial trigger points.[5] MT also has minimal side effects, no drug interactions, is low cost, and often includes positive patient-practitioner relations (which lead to a positive and productive mentality during therapeutic treatment and rehabilitation).
2) It does work. But how?
MT that successfully releases trigger points includes ischemic compression and friction massage. Ischemic compression involves holding pressure steadily on a trigger point until it softens/releases. Friction massage involves sliding the finger/hand/etc. along a (usually) venous direction of a muscle. This creates a vacuum/suction effect upon the circulation which quickly introduces freshened circulatory fluids to the area, and moves inflammatory chemicals present back into general circulation.[6] The freshened circulatory fluids include blood and lymph, which carry pain-relieving endorphins, as well as energy constituents for metabolic recovery for both the myofascial tissue and the neuromuscular junctions. Inflammatory chemicals removed include substance P, prostaglandins, bradykinin, etc.[7]
(image: Dry Needling & Manual Trigger Point Therapy Courses and Training)
If you’d like to see some of this for yourself, try this: locate the blue (venous) lines on the underside of your wrist. Press, then rub, slowly along the blue line toward the elbow. The blue line will go clear for a moment, then the blue, or venous, blood will return in a second or two. You have just performed friction massage to the veins which will drain blood and lymph from the tissues it serves. These tissues may contain nociceptive (pain inducing) and/or inflammatory biochemicals. If you flush the tissue of venous blood/lymph, creating a “quick-refresh” of arterial blood, the tissue will be flushed of painful biochemicals, while receiving pain-relieving biochemicals. This is the function of ischemic compression and friction massage for painful areas, including tissue with active trigger points.
3) How many sessions does it take before you feel relief?
If you have been properly diagnosed with MPS, and your practitioner is well-trained and experienced, you should feel immediate relief. Ischemic compression and/or friction massage releases a trigger point (and the attendant pain and tension) within a minute or two. If trigger points are extremely active, it may take several passes over an area to treat it completely.
There is a clinical understanding in our profession: the complex part of therapy is not releasing the patient’s pain (if you know what you are doing), but rather keeping them out of pain.
If your therapist is good, you will feel better, at least significantly, for a while. The task for you then is to:
- learn to do effective self-care to release the trigger points,
- stretch/strengthen the tissue, and
- track when the pain recurs, so that your practitioner can superimpose the timeline of recurrence with functional tasks, to possibly trace those tasks that need to be modified or eliminated (which will remove the trigger point’s perpetuating factor).
When these have been accomplished, you should be solidly on the road to recovery. Progress often follows a “two steps forward, one step back” pattern, as perpetuating factors are gradually eliminated and the tissue rehabilitates successfully. How long that will take depends on many factors: your age, general health, metabolic factors, stress levels, fitness, ergonomic factors, daily functional tasks, diet, sleep, emotional state, etc. Your doctor and therapist should help you to minimize the impact of triggers, and also to bolster those areas of overall healthy living that need help. If symptoms don’t improve noticeably within several weeks, you should seek other opinions and help.
————————————
[1] “Etiology of Myofascial Trigger Points,” article on the National Center for Biotechnology Information, U.S. National Library of Medicine website.
[2] “Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: an application of muscle pain concepts to myofascial pain syndrome,” article on the Science Direct website.
[3] “Physiological and clinical changes after therapeutic massage of the neck and shoulders,” Article on the Science Direct website.
[4] “The Effects of Pressure Release, Phonophoresis of Hydrocortisone, and Ultrasound on Upper Trapezius Latent Myofascial Trigger Point,” article on the Science Direct website.
[5] “The muscular force transmission system: Role of the intramuscular connective tissue,” article on the Science Direct website.
[6] Myofascial Pain and Dysfunction: the Trigger Point Manual, pg. 86.
[7] “Changes in Blood Flow and Cellular Metabolism at a Myofascial Trigger Point With Trigger Point Release (Ischemic Compression): A Proof-of-Principle Pilot Study,” article on the Science Direct website.

What kind of doctor should I see if I have myofascial pain syndrome?
This answer is based on my 25 years of teaming up with Bay Area physicians to help patients with myofascial pain syndrome.
To see the most effective and well-educated physician for myofascial pain syndrome, you should see a physiatrist, especially one specializing in pain management. Some other options include:
- Physicians who specialize in occupational injury, as they seem to have greater training and understanding of myofascial pain syndrome, and
- An increasing number of neurologists and orthopedists who specialize in pain management.
The first step to finding the right medical professional will be to do your own research on your condition, and thereby make sure that you actually have symptoms that fit the profile of MPS. While an official diagnosis will need to be done by a physician, your self-education will (or should) be welcomed by the physician, as it will save them time.
Next, you will want to do a cursory search on Google and Yelp to determine which physicians state a specialty in MPS. There may be many, as physicians seem to be racing to learn proper protocol for MPS treatment right now. The primary physiatrist I knew at Stanford Pain Management Clinic spends about 65% of his time traveling to educate physiatrists in MPS. Once you’ve decided a doctor might be right for you, you can always call their office, and ask the staff if they treat myofascial pain syndrome. You can even ask how they do it; or you can ask the physician at the appointment.
If they reply, “We inject cortisone into the sore/tender area,” they are probably not well-trained, as this doesn’t address the taut band and trigger point.
As part of a team with the well-trained physician, my job is to get rid of as much of the active/latent trigger points as possible. If there’s something I can’t address (too deep, too active, etc.), they inject it, because IT WORKS. However, they also realize that you can’t do more than 4 or 5 at a go, because they are painful.
The internet and the phone are your friends. Don’t be afraid to use them in order to find the best doctor to help you. Good luck!
Why Does Touch Feel Good?
This is an extremely complex and interesting question. The answer is even more complex.
As mammals, and especially as primates, our bodies and minds have evolved to desire, seek and receive comforting touch. At every stage of our development as individuals, and as part of a community, it is inarguably healthy for our bodies and minds. It is, in fact, integral to our very survival.
I think that, in order for touch to feel good, it must meet two criteria:
- The person being touched is honestly receptive, in the positive sense, to that touch; and
- The person providing the touch has the intent to, on some level, provide “comfort” to the person they are touching. (This can have different connotations for different people in different situations).
“Let’s start at the very beginning; a very good place to start…”
Engaging in comforting touch is something that is a primal driving force for human beings and primates, in addition to all mammals, and (surprisingly) avians. For mammals, it begins in the womb, as the first sensory neural network develops. This neural network then continues as the basis for the development of the central nervous system. This system, of course, is key to experiencing touch, as we can’t feel what we are anatomically and physiologically incapable of feeling. This is shown in a study of warm, comforting touch between married couples [2]. We require comforting touch from the moment of birth, through the entirety of our lives, and even up to the moment of death. Whether we receive that touch or not has a great impact on our overall well-being.
A great deal of research has determined that our bodies and minds require such touch in order to function properly. However, the variables in development regarding neurotransmitter levels and cultural parameters involving touch are still being studied in depth. The neurotransmitter/hormone oxytocin has been dubbed both the “love hormone” and the “cuddle hormone”, because it becomes highly expressed in the brain during comforting and/or erotic touch. Endorphins, the “feel-good” neurotransmitter/hormone is also highly present during physical interactions that make us psychologically or physically comforted or “attended to.” [3]
The differing parameters of sensory sensitivity levels have been accurately and somewhat humorously depicted in the following educational pictogram of the sensory “homunculus”:
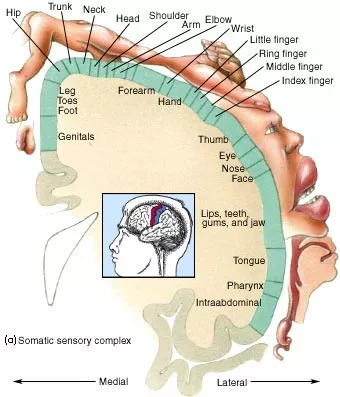
(Image credit: www.mhhe.com)
The human sensory net‘s “input parameters” are heavily loaded in favor of areas specifically developed and utilized in various stages of life, which translates functionally into sensory systems required for learning, and ultimately, survival.
What specific examples can be found in different stages of life?
As a fetus:
– touch of skin into the amniotic fluid, sac, womb, and surrounding/enveloping anatomy/physiology, to determine spatial parameters, due to the developmental nature of the integumentary (skin) system, in primary relation to the development of the central nervous system.
“From early days,
Beginning not long after that first time,
In which, a Babe, by intercourse of touch,
I held mute dialogues with my Mother’s heart
I have endeavour’d to display the means
Whereby this infant sensibility,
Great birthright of our Being, was in me
Augmented and sustain’d”
– William Wordsworth
The Prelude, 1850, II, 1. 265-272
As a newborn:
- Touch and smell, predominantly, of the mother (or whatever caretaker is most present)
- Rooting mechanisms in physiological/psychological reaction and behavior, in order to find FOOD
- Regulation of heat/cold independent of the mother
If any of these needs are not met, discomfort will result, and subsequent developmental, psychological, and behavioral complications will occur.
Through early life, ages 1-12:
Comforting touch is absolutely required for positive and functional development of the body and mind of the toddler, through to the adolescent. Positive, comforting touch from a parent or primary caregiver forms sensory feedback associations in the body and mind that set the course for positive inter-relational associations in their future, including dating, mating, sex, and parenthood. The effect of early comforting touch has been shown to help with early learning of physical comforting of friends, bonding of friends, development of communication with known or potential friends, and simple nonverbal, interpersonal communication (via facial expression and “body language”).
Early adulthood: ages 13-21:
At this stage, the young adult will have developed physical, psychological, and social awareness in relation to experiences gleaned from earlier stages of life. We are all works in progress. We take what we intuitively feel, then we take a chance via social experience, and then we process what happens. We either learn from these experiences or progress our awareness and forthrightness, or we become stuck in conceptual and social feedback loops – which can eventually “jump the fence” and progress anyways. Or not. These years are most often our first stages of sexual experience. If touch has not been recorded in our bodies and minds as “good” at this point, there’s trouble for the person. It can be changed, in one’s psyche, but the body is a bit harder to reprogram. Patience, understanding, and a willingness to affect change within oneself are paramount. It sounds trivial and easy, but it’s not.
Mature adulthood: ages 22-? (The next boundary in age is usually “senior”, age 60-70+, but it is variable):
These are the years when body awareness, habits, and customs reach their fruition through repetition. We are hopefully “comfortable in our own skin”, physically, psychologically, and socially. We not only rely on the ingrained senses of self and familiar patterns of interaction with others in order to survive and mature, but we also, as parents, are in the position to set the stage for our children in the same stages we ourselves have gone through. In fact, these experiences are so ingrained, not only in action and thought; they have made their way into common parlance of everyday experiences. Consider the phrases, “Rubbing people the wrong way,” “Having a prickly or abrasive personality, or alternately, a soft touch, or magic touch,” “Someone having to be ‘handled with kid gloves,’” “Someone being touchy, or thick/thin-skinned,” “Someone being ‘out of touch’ or ‘having lost their grip.’” Even a deeply “touching” experience is described also as “poignant (Middle English directly from Old French “poindre,” by way of Latin “pungere,” meaning to prick or touch). Metaphor for touch in language is deeply ingrained in us. Why? Because language is one of our main ways to communicate our experiences as a person.
Which also leads to the obvious: SEX and the human experience.
“Sex has been defined as, ‘the harmony of two souls and the contact of two epidermes.’ This elegantly emphasizes a basic truth: the massive involvement of the skin in sexual congress. The truth is that, in no other relationship is the skin so totally involved as in sexual intercourse. Sex, indeed, has been called the highest form of touch. In the profoundest sense, touch is the true language of sex.” [4]
“For touch,
Touch, by the holy powers of the Gods!
Is the sense of the body; whether something makes its way in
Or when a thing, which in the body had birth,
Hurts it, or gives pleasure issuing forth
To perform the generative deeds of Venus.”
-Lucretius (c. 96 B.C-c. 53 B.C)
De Rerum Natura, II, 434
If sexual intercourse did not feel as compelling and stunningly good as it does (or can), we would have long ago become extinct.
*And in our final years, the contacts we have grown to cherish and need from ourselves and all our family and communities, in our deepest being – physical, psychological, and social, will fade, even as the memory of its pleasures will be a secret fire in the deep recesses of the mind.
[1] Touching: The Significance of the Human Skin, Ashley Montagu, 1986
[2] Page on lww.com “Influence of a “Warm Touch” Support Enhancement Intervention Among Married Couples on Ambulatory Blood Pressure, Oxytocin, Alpha Amylase, and Cortisol”
[3] Behavioural function and neurobiological mechanisms
What is the purpose of the navel in the human body, beyond birth?
As Lou Davis says, there is no function of the navel for autonomic function past birth. But it can be argued that there is a musculoskeletal / myofascial function to the navel as it relates to deeper muscular and connective tissue structures in relation to anatomical development and subsequent physiological functional capacity.
The navel is a connective tissue (fascia) locus[1] that is centered around our physical center of gravity, which is why physiotherapists make such a fuss about “core” strengthening. The abdominal muscles and associated connective tissue (including in the area of the navel) constitute a center of support for the viscera and the musculoskeletal (including Lumbar) structures surrounding and supporting it.
This becomes important, in physiotherapy, when the “core abdominal support” has been anatomically or physiologically / functionally compromised. The navel itself doesn’t have muscular components, such as contractive sarcomeres, but it affects the sarcomeres of the surrounding myofascia, including rectus abdominus and external obliques,etc. The navel itself is not the issue, but its location at our center of gravity and the functionality that extends from that center of gravity is the issue.
[1] Fascia: The Tensional Network Of the Human Body; 2012, Elsevier; Robert Schleip, Thomas Findley, Leon Chaitow, Peter Huijing; pgs. 50-52

What is the best thing to do if you burn your hand?
Any burn that is 2nd or 3rd degree (puckering or blistering/charring of the skin) needs to be seen to by a physician asap. Otherwise, you risk serious, possibly life-threatening, infection and loss of bodily tissue.
In cases of a simple first-degree burn or scald (quick touch to a heated surface or liquid), you have to cool the skin temperature to normalize it as quickly as possible. This is best-done by running the burned/scalded skin under cold running (clean) water until the first “burning” sensation has reduced or passed (at least for one minute). This will also hopefully clean the wound of any foreign substance, such as charred material or chemical irritants.
Next, you want to disinfect and numb the tissue, both to prevent infection from the compromised area (cohesive skin is the most powerful exterior barrier to infection our body has) and to numb the area’s nerves that perceive burning pain. This helps to abate the hyper-inflammatory process that can result from sudden tissue insult, such as a burn.
This can be achieved in several ways. The easiest is to apply a combination disinfectant/numbing ointment such as Neosporin “with Pain Relief” (lidocaine). The disinfectants, combined with the topical numbing agent lidocaine, help the metabolism of the tissue resist infection until the skin (dermis layers affected) has healed sufficiently to do so unaided. Aloe Vera gel has also been used as a demulcent (skin-soother) since antiquity, and you can add this after the disinfectant/numbing agents.
There have been many herbal agents throughout history that have been utilized to provide the disinfectant, numbing, and demulcent (skin-soother) properties described above. However, any encompassing list and history of these agents would make this answer far too long, especially when there are cheap and effective alternatives available at the supermarkets and corner stores.
Once you have treated the wound with good cooling, disinfecting, numbing, and demulcent agents, you need to cover the wound with some sort of sterile dressing. Usually this means – Yes! – a Band-Aid. Think of the Band-Aid dressing as a kind of “temporary non-adhesive synthetic skin” that will serve as a protective barrier while your actual skin is vulnerable and healing. Make sure that the adhesive doesn’t touch the wounded skin, or it will abrade the skin further. You will want to repeat this treatment every 4-6 hours as needed, for at least 24 hours: rinsing, applying “ointment” and covering with a bandage. If there is ANY indication of excessive reddening, swelling, or sensations of itching, burning, etc., see a doctor (emergency, if necessary) immediately. This is no joke – burns can be very dangerous!
If no adverse effects are noted, a kiss to the (bandaged) boo-boo may help too!
What does where the pain lies tell you about the nature of a headache?
Most headaches around the eyes, cheeks, temples, and top, back or base of the skull involve the muscles, connective tissue (myofascia), nerves or structures around the joints of the jaw, ear, and/or sinuses. These headaches can be primarily caused by a direct strain or sprain, or secondarily caused by drug side effects or other conditions that precipitate inflammation in those areas. The brain tissue itself does not have nerve endings that perceive pain, but the tissue surrounding it certainly does!
There are many muscles in the neck and head. I’ll primarily address the myofascial pain pattern of each one, since their are too many related conditions and drug effects to list in a single answer. In any case, a thorough examination by a physician to determine the cause of the pain would still be called for.Areas of pain in muscles (from Travell and Simons’ Myofascial Pain and Dysfunction, volume I) are grouped into the following areas:
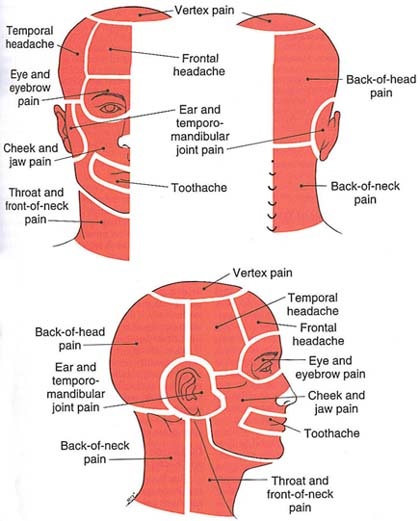
(Ch.5, pg.167)
The muscles that create the referred pain in these areas are grouped here, in the same text:
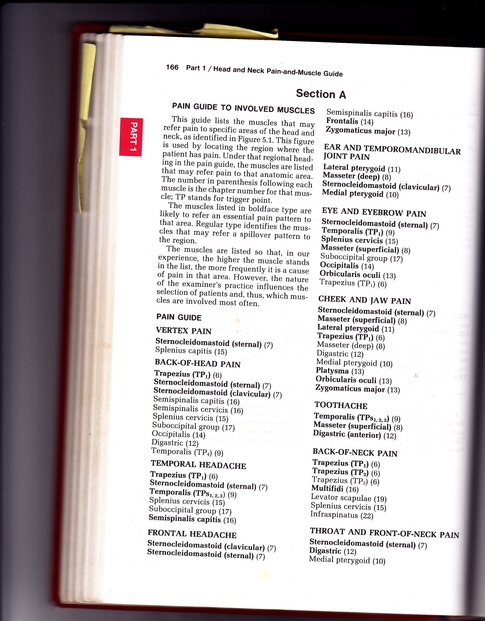
If you are curious about the specific pain pattern of a particular muscle, you can visit this site (or other similar accredited sites) to find out: National Association of Myofascial Trigger Point Therapists.
For the temporalis muscle, a sample pattern might look like this:
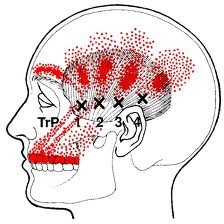
Muscles of the neck can refer pain locally or up into areas of the head, including the face and jaw. Most facial muscles (including muscles of the eye, ear and jaw) tend to refer pain very locally; they very rarely refer down to the neck.
Pain in the face and jaw, especially, tend to indicate problems with the sinuses, eyes, muscles of mastication (chewing), dental problems (such as malocclusion or infection), or some other local infection (such as a cold or flu). Pain can be triggered by any recurrent infection or source of inflammation, even cancer. This essentially means that therapy for the muscles may provide temporary relief, but since the primary trigger has not been resolved, it will keep recurring.
If the problem is primarily myofascial, correction of any source of mechanical strain (including postural or ergonomic strain) must be removed or at least reduced for the therapy to be effective and lasting.
The first 3 books on this list are my favorites on non-migraine headaches for the layperson: Amazon.com: trigger points and headache: Books
BUT, of course, if a headache is especially severe, has lasted for longer than three days, happens repeatedly, is interfering with your functioning significantly, is affecting your eyesight, hearing, balance, cognitive function, or is doing anything other than just making your head hurt, please go see a doctor right away!

What do you do to stay productive all day?
The answers to this will be a bit subjective, due to the demands and personal makeup of our different lives. As a 46yo woman, wife, mother, business owner, muscle therapist, etc., here are some things that help keep me on track.
- Good sleep. This cannot be overstated, and I am fierce about not only the quantity (min. 6 hours, 8 best), but the quality. I spend an hour with a hot bath and soothing music and meditation to calm my body and mind down before going to bed. I have a great bed and pillow, and I make sure that I am warm and comfortable during sleep. Consequently, I fall deeply asleep about 2 minutes after hitting the pillow, and I wake up when the alarm goes off, refreshed and ready for the day. Well, after one cup of coffee.
- Morning exercise. I have a pretty rigid schedule, but I find that 30 minutes of morning exercise (minimum) in a natural setting, such as a walk on the beach (or somewhere similarly enjoyable) clears away the “cobwebs” physically and mentally, and I feel like it gives me a jump-start on increased energy for the rest of the day. It clears my mind of clutter and makes me feel ready to face the day’s challenges calmly. It works better for me first thing in the morning, because I tend to be too busy or tired later in the day, when it’s easier to blow off.
- Good nutrition. I have high physical and mental demands on me during my workday, and I am sensitive to drops in blood glucose levels (runs in my family). I try to get good quality food (nutritious, moderate fat/sugar/salt intake) at even 2-4 hour intervals throughout the day. Low-fat protein sources, such as soy milk or miso, tend to help me stay awake and alert.
- Productive use of downtime. I have been trying to make a habit of meditating for up to 15-minute intervals through the day during “waiting” periods. These can include the time between appointments, end of the workday, during a bath, etc. Allowing myself to try to “drain of thought” is like a deep breath of refreshing air for my whole self. Which leads me to:
- Take notes. I have always found it difficult to give myself permission to jot down a note (on paper, Post-its, Evernote, my wrist, etc.) to remember something trivial (calling a friend, picking up something at the store, etc). I do not remember these things well while working. When I’ve written the note, I no longer feel the weight of trying to remember, and I can concentrate better on the moment at hand.
- Regular time with family and friends. We make a family habit of eating together and watching a movie together every night. Yes, every night. This requires a fair bit of compromise on all our parts. We have never regretted it, and you don’t ever get the time with your kids back to do over. It makes for a grateful, peaceful evening. As regularly as possible, we try to get together with friends about whom we care deeply. Scheduling ahead helps. Again, we’re never sorry we did, and good times and lasting friendships are shared by all.
Rinse, repeat.

How do sports medicine physicians (MD or DO) and physiotherapists view chiropractic?
My perspective on chiropractic, outlined below in 3 parts, is that of an advanced muscle therapy practitioner who has worked with many wonderful DCs in the Bay Area. We’re lucky to have them and their services.
1. How do sports medicine physicians (MD or DO) and physiotherapists view chiropractic?
This will depend heavily on which MD/DO you ask, their professional training, and the focus of their practice. Those that specialize in pain medicine are often acquainted with experienced DCs that are very skilled in helping people get out of pain very quickly. Chiropractors have a very in-depth training in musculoskeletal anatomy and physiology that enables them to understand and enlist effective therapeutic techniques that can achieve speedy relief from symptoms. The proof is in the result: does the patient feel better, or not? Although no technique is a panacea, a DC’s techniques often yield an answer of “yes.”
In my 24 years of experience, I’ve found that sometimes you need someone skilled to cavitate a joint (therapeutically manipulate the alignment of the bony tissue), or series of joints, if they are “stuck.” You have to take into account the tension and function of soft tissue as well (perhaps even primarily), but if the joint is “stuck,” it needs to be mobilized, softly and mindfully. It won’t be functional otherwise, and therapeutically, that’s the bottom line.
2. Has chiropractic managed to shake itself loose from the old Palmerian dogma of “subluxations” and the notion that “adjustments” can cure all manner of illnesses?
As far as I know, DC curriculum still includes such dogma. However, any responsible practitioner knows that no technique is a panacea, and answering on behalf of those DCs who no longer subscribe to such notions, and whom I respect, the answer is “Yes.”
Good DCs have many therapeutic techniques besides “adjustments.” When used well, they get great results in pain management.
There are many symptoms and conditions where cavitation can help provide comfort. See also this entry on Quora.com: Human Physiology: Is it okay to pop/crack your joints (knuckles/back/neck/etc.) daily?
3. How prevalent are chiropractors in sports medicine?
Again, this will depend on the area of practice and training standards. If someone is good at what they do (getting people out of pain and back to functional levels), they could be an MD, DO, PT, DC, or MT. “Therapy” is a very divergent and fluctuating field, one that has only one goal: Get Someone Better, ASAP. The trick is, the modality must be consistently effective and reproducible. As in any therapeutic field, great DCs are well-educated healers. They will most probably be at the forefront of challenging cases, providing pretty astonishing results. I’m honored to be working with some of the best of them. They continually, delightfully, surprise me and my patients with results that we can’t get from soft-tissue therapy or medications alone.