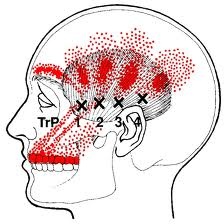
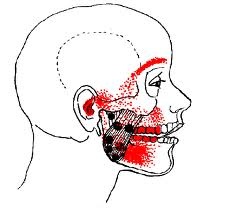
“Muscle knots,” otherwise known as trigger points, can occur in any muscle of the body when that muscle is used improperly or damaged. With repeated misuse or damage, the affected sarcomeres (contracting fibers) can “lock” into immobility and inflammation of varying levels. Online research of any skeletal muscle of the body reveals images of trigger point pain patterns for that muscle. (Various muscles associated with locations of pain throughout the body are shown here too: National Association of Myofascial Trigger Point Therapists | Symptom Checker)
Current wisdom on this subject is as follows: “The presence of CGRP (calcitonin gene-related peptide) drives the system to become chronic, potentiating the motor endplate response and potentiating, with SubstanceP, activation of muscle nociceptors. The combination of acidic myofascial pH and proinflammatory mediators at the active trigger point contributes to segmental spread of nociceptive input into the dorsal horn of the spinal cord and leads to the activation of multiple receptive fields. Neuroplastic changes in dorsal horn neurons occur in response to constant nociceptive barrage, causing further activation of neighboring and regional dorsal horn neurons that now have lowered thresholds. This results in the observed phenomena of hypersensitivity, allodynia, and referred pain that is characteristic of the active myofascial trigger point.” 1
To put it in simpler clinical terms, an active trigger point that is referring pain will activate (as a result of tissue metabolism and biochemistry altering the nociceptive threshold) associated soft tissue and neural regions through neuroplasticity.
1. An expansion of Simons’ integrated hypothesis of trigger point formation (pg. 474, 1st P.)