From a reader:
Why am I getting headaches when I make long phone calls? Why do they last up to a week before the pain starts to go away? It’s hard to get to sleep with such pain, and even when I do sleep, the pain is still there when I wake up. Is this dangerous for me? Are there any health concerns?
My answer:
First, you should definitely see a physician. Make that appointment ASAP! 😉
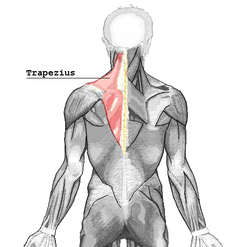
That being said, a likely scenario is activated trigger points in the muscles of the neck and shoulder (most likely the upper trapezius, splenius capitus, splenius cervicis, and suboccipitals). These are the muscles that produce this very familiar posture:
How often do we see and DO this on any given day? This action strains the muscles and the connective tissue (myofascia) mentioned above because they are probably not used to, and are definitely not “designed for,” the sustained contraction shown above.
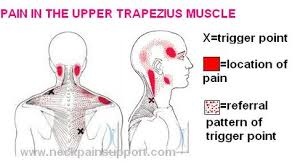
Let’s go through the pain patterns that emerge when these various muscles undergo repetitive strain (which leads to active trigger point referral patterns):
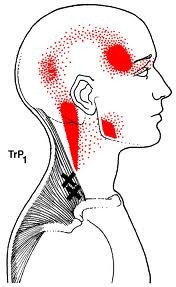
1) Upper trapezius:
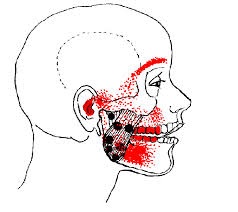
2) Splenius capitus:
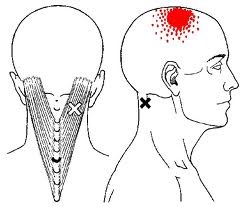
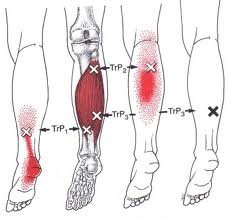
3) Splenius cervicis:
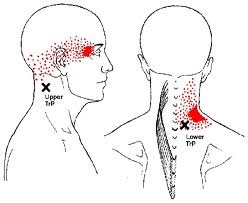
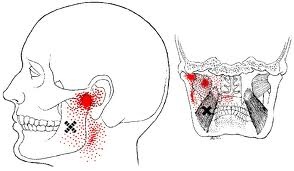
4) Suboccipitals:
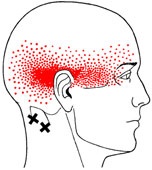
(Credit for all of these medical illustrations belongs to Barbara D. Cummings, the illustrator for Travell and Simons’ “Trigger Point Manual.” She had an extraordinary gift for giving the viewer an accurate, literal view of subjective pain.)
ALL of these muscles are engaged in the posture in the first picture, where someone is holding a phone between their head/ear and their shoulder. You have to hold it there somehow, right? Well, these are the muscles that do it for you, and they are most probably strained and activated through prolonged, static holding of this posture.
The most obvious way to help prevent this from happening again is by correcting the problematic posture that strains these muscles:
-
Keep your head upright and your neck straight on prolonged conversations.
-
Switch which hand holds the phone, so that you are not constantly loading the same muscles on the same side (thereby straining them). Give them a rest by using the similar muscles on the opposite side, then switch again when they get tired.
-
Give yourself a few moments to slowly take your head and shoulders through their comfortable range-of-motion, in order to restore circulation and re-establish normal resting length for the muscles. This involves making SLOW circles, or moving the head in opposing directions (i.e., up/down & right/left).
Also, if the calls tend to be especially stressful, give yourself “breaks” every 5-10 minutes to disengage for at least 60 seconds. If needed, perhaps mention that you must take a moment to attend to something personal (letting the cat in, a call on the other line, etc.), then take that moment to:
-
Consciously relax any tension you feel. For example, try tensing your muscles for 5 seconds while holding your breath, then exhale while relaxing those muscles (2-3 times in a row). This is a simple biofeedback technique.
-
Imagine the tension as something physical (smoke, dirty water, etc.) draining out of your feet into the floor/ground. This is a simple meditative/visualisation technique.
-
Give yourself permission to drop as much tension as you can, and to breathe as slowly, deeply, and as relaxed as you can manage. This is a simple cognitive behavioral therapy technique.
When ready, resume conversation. 🙂
If you would like to know some relatively easy ways to relax your muscles and stop the pain, and your physician has cleared you to do such exercises as the above (no contraindications), see my blog post How can I reduce knots in my shoulders (trapezius muscles)?
Good luck, truly. I think a great deal of people are struggling with this right now.