This is a hot topic in physiotherapy, so I’m adding some research and detail to this. If you’re looking for a quick answer, see the first three points, because I agree with them. For those who want more data, I provide further detail to the symptom/diagnosis below.
The generally accepted characteristics of Delayed Onset Muscle Soreness (DOMS) are: [1] [2] [3] [5]
-
generally due to unusual or unaccustomed muscular activity (What did you do that was new or different?)
-
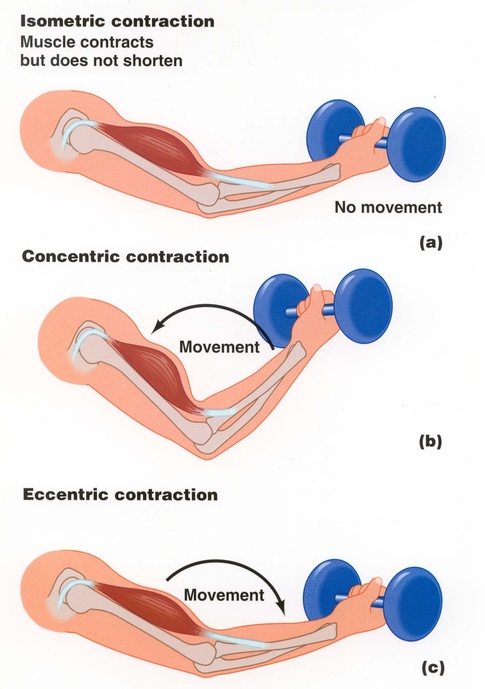
most often associated with eccentric (lengthening) contraction versus concentric (shortening) loading. For example, when your torso returns slowly to the floor after a sit-up (eccentric for rectus abdominus) versus the sit-up itself (concentric for rectus abdominus). Another example is lifting and lowering a barbell using your biceps:
-
general period of onset is 24 hours or so after exercise-incident, peaks around 24-72 hours after exercise-incident, and then mostly subsides (versus a muscle/tendon STRAIN or ligament SPRAIN, which continues beyond this timeline).
The two major associated theories for DOMS:
-
“The view taken here (see also Morgan & Allen, 1999) is that the damage process begins with overstretch of sarcomeres. [1]
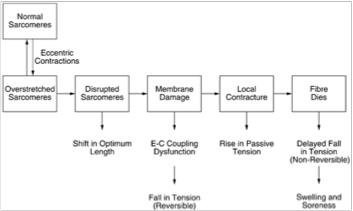
“Postulated series of events leading to muscle damage from eccentric exercise:
- During an active lengthening, longer, weaker sarcomeres are stretched onto the descending limb of their length-tension relation where they lengthen rapidly, uncontrollably, until they are beyond myofilament overlap and tension in passive structures has halted further lengthening. Repeated overextension of sarcomeres leads to their disruption.
- Muscle fibres with disrupted sarcomeres in series with still-functioning sarcomeres show a shift in optimum length for tension in the direction of longer muscle lengths. When the region of disruption is large enough it leads to membrane damage. This could be envisaged as a two-stage process, beginning with tearing of t-tubules. Any fall in tension at this point would be reversible with caffeine (see text).
- It would be followed by damage to the sarcoplasmic reticulum, uncontrolled Ca2+ release from its stores and triggering of a local injury contracture. That, in turn, would raise muscle passive tension. If the damage was extensive enough, parts of the fibre, or the whole fibre, would die. This fall in tension would not be recoverable with caffeine.
- Breakdown products of dead and dying cells would lead to a local inflammatory response associated with tissue oedema and soreness.”
(Source: The Journal of Physiology, Volume 537, Issue 2, pages 333–345, December 2001)
-
“The alternative view is that the starting point is damage to components of the excitation-contraction (E-C) coupling process. In a recent review, Warren et al. (2001) summarised their position by declaring that 75% or more of the decline in tension after eccentric exercise was attributable to a failure of the E-C coupling process. The remaining damage seen during the first few days after the exercise was attributed by the authors to physical disruption of the tension-bearing elements within the muscle. So the suggestion is that most of the primary damage arises in the E-C coupling system and only a small component occurs at the level of the sarcomeres. Supporting evidence comes from the observation that in mouse muscle the post-exercise deficit in tension can be recovered with caffeine (Warren et al. 1993; Balnave & Allen, 1995). In the first of these studies, tension was recovered with 50 mm caffeine, which releases Ca2+ from the sarcoplasmic reticulum and leads to development of a contracture in the muscle. In the second, 10 mm caffeine was used to potentiate tension in single fibres in response to direct electrical stimulation. It was concluded that in mouse fibres changes in E-C coupling may be a major contributor to the observed fall in tension after eccentric contractions (Allen, 2001). [2] [4]
Neither of these theories will be resolved without:
-
a way to measure pain objectively, and
-
a way to measure the biochemical millieu of the area from “start to finish” in a controlled setting. This is a key area for fMRI studies.
What does it all mean??
Isometric contractions may not build hypertonicity (excessive tension) as quickly, but they will also produce less widespread micro-damage, with its resultant pain and inflammation lasting up to 4 days. This may allow you to resume continuing strengthening faster than if you concentrate mainly on eccentric strengthening. This does not make it less valuable, simply more dangerous to the user of new methods/exercises It also makes them more needful of longer recovery periods in order to avoid repeated and deeper strain/sprain.
[1] Delayed onset muscle soreness (Wiki)
[3] Eccentric exercise-induced injuries to contractile and cytoskeletal muscle fibre components