From a reader:
How can I reduce knots in my shoulders (trapezius muscles)? I work at a computer most of the day, and have tight knots in my shoulders; specifically, in my trapezius muscles. How can I reduce the tension in these muscles, without having someone else massage them? Are there self-massage techniques I can use? What are appropriate stretches?
My answer:
EVERYBODY gets tension (and sometimes, pain) in the neck and shoulders as well as in between the shoulder blades. This has, of course, increased in these times when we’re all looking down and hunching up at our phones and laptops. Here’s how to get rid of it. Based on the reader’s questions, I’ve broken up my answer into 3 sections below.
How do I reduce tension in these muscles?
This is the most important question. You could have the best therapist to resolve the tension for a time, but if you continue to do the actions that result in the tension and pain, they will just keep coming back and probably keep getting worse.
The most common problem that exacerbates tension and pain in the neck and shoulders is holding the neck in an unnatural position. The two most common are looking down for extended periods and craning the neck and head forward (most probably to focus on miniscule print on a device such as a smartphone or laptop). The answer is to figure out how to keep the head as upright and without rotation as possible, while you relax your shoulders and arms at your sides.
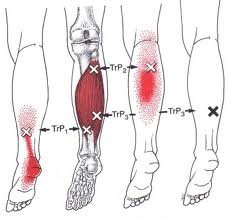
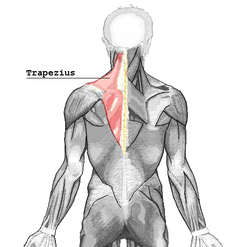
The trapezius itself is, ironically, not the most common cause of neck/shoulder pain in the curve of the shoulder (the levator scapula is). However, TrP1 (Trigger Point 1) at the curve of the neck/shoulder is one of the myofascial TrPs observed the most often [1]:
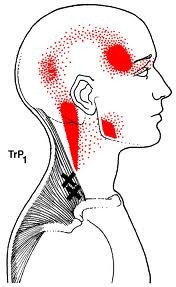
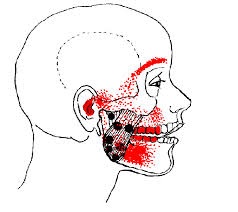
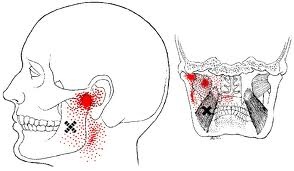
There are about seven common trigger points located in the upper, middle and lower portions of the trapezius muscle:
Point 7 (x) produces pilomtor activity or “gooseflesh” to the upper extremity [2]
“In study of static loading, Bearns (1961) discovered that the upper fibers of trapezius, contrary to universal teaching, ‘play no active part in the support of the shoulder girdle in the relaxed upright posture.” [3]
Are there self-massage techniques I can use?
ABSOLUTELY.
FIRST, you must have been assured by a proper diagnostician (MD/DO) that there are no problems (such as a herniated disc, bone spurs, etc.) that will constantly madden the nerves that feed the musculature of the neck and shoulder. If there is such an inflammatory component, anything I write here will be transitory because the true cause has not been addressed. My suggestions below can temporarily interrupt the pain signal, which has benefit, but ALL pieces of the problem must be addressed to have lasting comfort.
First, it is very helpful to heat the area first. This will dilate blood and lymph vessels, bringing an influx of fresh blood into the area. It will also soften the connective tissue (fascia) that surrounds and binds the muscle fibers and heads, which will make the whole area more amenable to stretching. This step also prepares the tissue for massage (flushing) of the inflammatory chemicals that are making it hurt.
You can use a couple Swedish massage techniques to soften and relax the tissue. These are friction (rubbing along the fiber) and kneading (like with bread dough). For more information, see my blog entry What is the difference between kneading, rolling, percussion, and vibration?
For trigger point deactivation, you can use point-compression with fingertip(s) or a pressure tool (such as a backnobber or theracane):

You can also use a tennis or pinky ball against a wall, but they are notoriously difficult to use on the curve of the shoulder. I’ve found the backnobber to be the most useful. It’s only $30, and the product and subsequent comfort can last the rest of your life (no affiliation, just a big, big fan of one of the coolest designs EVER!) [4]
Here’s what you do:
-
Find the trigger point (any “x” in the above diagrams) that produces the pain pattern that you have, or alternately find a knot in a band of muscle in the curve of the neck/shoulder.
-
Heat first!
-
Apply pressure with a fingertip or tool, just enough to “feel it,” and HOLD for 15-60 seconds, until it feels like it is “dissolving/softening,” or until it feels “done.”
-
Apply the same technique to adjacent and associated trigger points
-
At this point, you MUST take the muscles released through their normal resting range of motion!
What are appropriate stretches?
This is a tricky one for the neck and shoulder, which have an astonishing array of motion capabilities.
PLEASE NOTE: The exercises below will NOT help and will probably be painful and/or harmful if the tissue is not softened first. Before doing any of the below stretches, follow steps 1 and 2 above. Take it slow and EASY, and remember to breathe. Do NOT make it hurt, just stop at the first point of stretch and relax into it.
Stretches that are most helpful for neck/shoulder pain are as follows:

(points 4-7)

(points 5-7)

If you follow the steps above, you should get immediate, long-lasting relief from neck/shoulder pain from computer use. If you do not, it’s time to see a pain-management doctor. Don’t wait. The longer these muscles go on in an inflamed, irritated, shortened state, the longer it takes to deactivate and rehabilitate them.
Ultimately, the triggers must be eliminated, the tissue must be softened/relaxed/deactivated, and then it must be strengthened within its current capability.
[1] Myofascial Pain and Dysfunction; the Trigger Point Manual, Travell and Simons, pg.184
[3] Muscles Alive; Their Functions Revealed by Electromyography, John V. Basmajian, Carlo J. DeLuca, pg.266