All the different useful procedures of massage can be classified under eight main categories.
Passive Touch is passive (still). It consists of lightly touching the body with one or more fingers, the whole hand or both hands. This technique is used in Swedish massage, Myofascial Release and Craniosacral therapy, to name a few. Physiological effects include elevation of temperature via heat from the hand, and sensory influence on the cutaneous nerves, often associated with comfort.
Simple touch can be remarkably effective in relieving hypersensitivities, especially in the head and joints. Nervous irritability can be quieted sometimes by simple touch of the hand on the head.
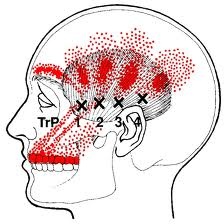
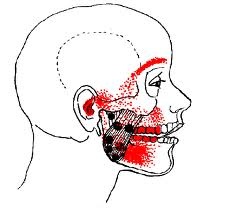
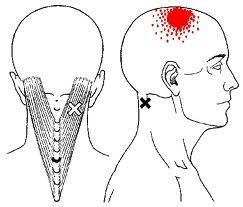
Compression consists of making light or heavy pressure with the whole hand or one or more fingers. This is used in manual deactivation of a myofascial trigger point or to temporarily numb an irritated nerve such as in trigeminal neuralgia or sciatica. When administered correctly, the effect of compression is to diminish swelling and circulatory congestion, and to slightly numb the nerves pressed upon.
Stroking is simply light touch combined with motion. The tips of two to five fingers or the entire palmar surface of one or both hands are moved slowly and gently over the skin with minimal contact at a rate of 1-2 inches per second in the direction of arterial (heart-outward) flow only.
There are many different techniques and reasons for stroking, both direct and reflex. The main effect of stroking is a decided sedative effect. However, very light stroking may produce a very powerful reflex effect, like a tickle or stimulant to spinal nerve roots. This can be very useful to alleviate sleeplessness or hypersensitivity such as a nervous headache (very useful with upset babies and children). Neuralgic pain and numbness may also be somewhat abated with this technique. It can be used abdominally to reflexively stimulate digestion: think of how you gently rub your stomach when you have overeaten or have indigestion.
Friction is where the whole or part of the hand is moved steadily over the surface of the skin following venous flow (toward the heart) with a varying but significant degree of pressure according to the “thickness” of the area being worked on. There are many different techniques for friction depending on the influence you want on the tissue. As a rule, some lubricant such as oil, lotion or powder should be utilized to avoid overstimulation, abrasion and irritation of the skin.
The principal objective of friction is to encourage better circulation, thus emptying the veins and lymphatic spaces and channels of waste matter and painful chemicals. It is probably the most valuable of the various massage procedures.
Swedish massage, Cross-Fiber massage and Active Release Technique use deep friction to break up scar tissue in different structures such as skin, muscle, tendon or ligament. Manual Lymphatic Drainage uses very light friction to clear swelling and congestion from joints and lymphatic outlets.
Friction and kneading are probably the most widely used massage techniques worldwide.
Kneading is probably the best known massage procedure, as familiar as kneading dough. It essentially consists of alternating and intermittent compression and squeezing of the tissue, either by grasping it or compressing it against underlying bony surfaces. Kneading differs from friction in that the skin is held in firm contact with the surface of the hand.
Kneading techniques can either be superficial or deep, and can be further delineated by specific techniques. These include superficial/deep kneading (like a baker kneads dough), skin rolling, wringing, and palm/fist/finger kneading, to name a few. Swedish massage and Deep Tissue Massage utilize these heavily. The main goal of kneading is to stimulate all the vital activities of the body part being worked on, including the nerves, blood vessels, glands and cellular exchanges of the tissue. Deep kneading assists muscles to increase in size and function through better circulatory exchange, and assists in the removal of painful chemicals and connective tissue adhesion. Superficial kneading is especially indicated for swelling and any other condition where the skin and superficial circulatory channels need to be more active.
Vibration consists of fine vibratory or shaking movements from the therapist’s hands to the area worked on. This can be subdivided into lateral, knuckle, superficial, deep, shaking and digital vibration, depending on how the therapist uses his or her hands to address the patient’s needs.
Vibration primarily stimulates. It can cause muscle contraction, a pleasant tingling sensation due to stimulation of sensory nerves, and increased blood flow and subsequent temperature rise of the region. It is valuable in cases of paralysis, neuralgia or neurological weakness or fatigue, where stimulation of the area’s function is needed. I have found it to be especially helpful in cases where the patient is unable to relax a muscle or has trouble with neurologic dysfunction and spasm (such as with Cerebral Palsy).
Percussion consists of blows to the tissue using the hands or fingers with varying degrees of technique and force. The movement is always elastic and from the wrist, which penetrates deeply without bruising superficial structures. As a rule, the hand should strike the body transversely across the muscle’s fibers. Different techniques include tapping strike w/ finger’s ends, spatting (strike w/ fingertips), clapping (strike w/ whole palm), hacking (strike w/ pinky side of hand) and beating (strike with palmar side of a closed fist).
Percussion is a powerful stimulant for both the skin and underlying structures. A short, light application produces a momentary spasm, and thus blanching, of the superficial vessels. Strong percussion dilates the vessels a great deal, as evidenced by the reddening which follows. If very strong, percussion can produce nerve paralysis, as any martial artist knows. Other effects include stimulation of the organs through reflex centers and the spinal cord, and assisting with dislodging mucus congestion in the lungs.
Joint Movement obviously consists of the therapist moving the patient’s joint through a range of motion. This can be combined with other techniques such as deep friction (as in Active Release technique) or touch (as in Myofascial Release and Unwinding). It may be either passive (no effort from the patient) or resistive (as in Proprioceptive Neuromuscular Facilitation, Lewit technique, etc.). Joint Movement strongly affects fluid flow through both the joint and the joint’s connective and adjacent structures. It is useful in cases where there is stiffness, pain, swelling and hyperstimulation. Think of how you shake your hand when it feels tired or stiff.
All this being said, reading this or any other blog does not make one a massage therapist. If you want to truly learn these techniques, whether to give a better backrub or to become a licensed therapist, check out good schools nearby and take an appropriate class. The internet and certifying massage school associations, such as AMTA (American Massage Therapy Association), can help with this. The skills gained will benefit you and your loved ones throughout your lives.
There are many wonderful books about massage, but my favorite one on basic technique is “Art of Massage” (John Harvey Kellogg, MD, reprint 1975 by Health Research, CA), which was our main textbook in 1988. Most of the information on our Medical Board exam for licensure was taken from this text.